

Most “how fast will this work” articles measure one thing: the benefit. That is half a scorecard. A complete grade needs to track cost on the same clock as benefit, because in the actual trials, both were running simultaneously. Below is the rubric this piece uses, applied without rounding in anyone’s favor.
The rubric
Four criteria, scored against published data only:
- Time to a statistically significant benefit. How many weeks until the trial data shows a measurable effect.
- Time to the first documented harm signal. How many weeks until suppression, injury, or dysfunction shows up in controlled or case-report data.
- Product integrity in the retail market. Does the thing sold online actually contain what the label says, at the labeled dose.
- Availability of a monitored path. Can a licensed clinician prescribe and track this compound at all, or does “supervision” not exist for this category.
Each compound class gets scored against all four. No partial credit for good intentions.
Criterion 1: time to benefit , SARMs
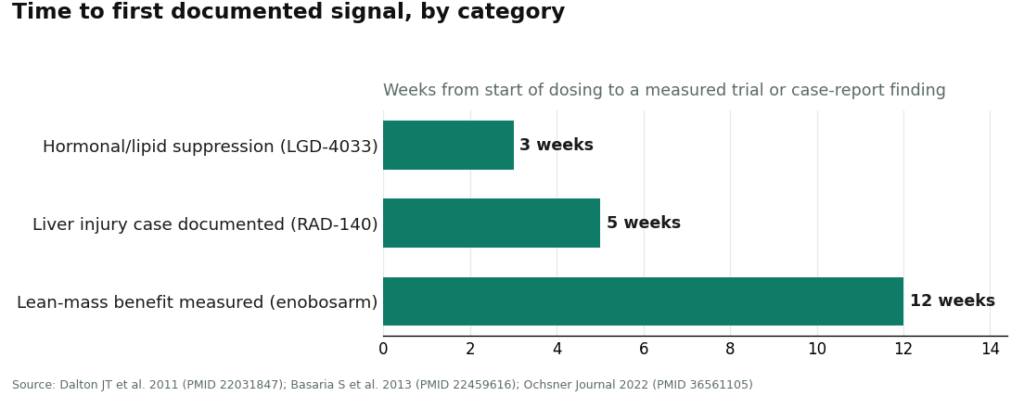
The reference data point here is a phase 2 trial of enobosarm (ostarine): 120 healthy elderly men and postmenopausal women, double-blind, placebo-controlled, 12 weeks. Result: dose-dependent, statistically significant increases in lean body mass (P less than 0.001 at the 3 mg dose against placebo), plus measurable gains in physical function [P1].
Score: real, positive, and dated. Twelve weeks to a documented signal is not nothing. Write it down as the strongest entry on the benefit side of the ledger.
Caveat, and it matters: this number was produced under monitoring, with a known manufactured product, inside a clinical trial. It is a benefit timeline for that specific, verified compound. It does not transfer automatically to a vial purchased online, and it says nothing about what happens past week 12.
Criterion 2: time to harm , SARMs
Three separate data points land here, and none of them wait as long as the benefit did.
Hormonal suppression: in a controlled trial of LGD-4033, 21 days of dosing (the source text also states this as three weeks) produced dose-dependent suppression of total testosterone, sex hormone-binding globulin, and HDL cholesterol in healthy young men [P2]. Three weeks. That is nine weeks ahead of the enobosarm benefit checkpoint.
Liver injury: a published case report describes a 24-year-old man who developed cholestatic liver injury after five weeks of RAD-140, peak total bilirubin of 38.5 mg/dL, confirmed on biopsy [P3]. One case does not equal a population rate, and that qualifier stands. But five weeks is still seven weeks earlier than the 12-week benefit mark.
Regulatory summary: the FDA states that SARM-containing products carry the risk of life-threatening reactions including liver damage, along with increased risk of heart attack and stroke [P6]. That is not timeline data specifically, it is a standing warning, but it belongs in the same column as the other harm entries.
Score: on the available evidence, the cost side of the clock consistently runs faster than the benefit side. That is the asymmetry this rubric is built to surface, and it does not flatter the SARM category.
Criterion 3: product integrity , SARMs
This criterion determines whether any of the above timelines even apply to a given purchase. Researchers tested 44 products sold online as SARMs. Only 52% contained the labeled SARM. Of the ones that did contain it, the dose was wrong in most of them [P5].
Score: fails. A timeline is a function of dose times compound. If roughly half the sample either lacked the labeled compound or had the wrong dose, “what to expect by week six” is not answerable for any specific bottle. This criterion caps every other score in this category, because it undermines the premise that a timeline applies at all.
Criterion 4: monitored path , SARMs
The U.S. Anti-Doping Agency states plainly that there are no FDA-approved SARMs available for prescription [P4]. Every SARM in circulation is investigational.
Score: fails, structurally, not as a matter of degree. There is no version of “get this checked by a clinician periodically” for a SARM, because there is no clinician pathway to check against. A monitored route produces bloodwork, follow-up, and adjustment. An unmonitored route produces none of that, and the absence of monitoring does not slow anything down. It just removes the instruments that would have caught it.
Running the same rubric against peptides
The scoring exercise looks different here, and the difference is itself informative.
Criterion 1 (time to benefit): there is no single number to report, because “peptide” is not one category. Some are FDA-approved drugs with trial data specific to each drug and indication. Some are medications a licensed pharmacy compounds against a prescription, where the active ingredient is characterized. Some are research-status peptides with sparse human data, and any timeline claim for those should be read with the same skepticism applied to SARM protocols above. Score: not gradable as a single line item. Must be scored compound by compound.
Criterion 2 (time to harm): same answer. No single figure applies across the category.
Criterion 3 (product integrity): varies by acquisition route. A compounded prescription filled by a licensed pharmacy is a different integrity proposition than a vial bought off a forum. The source data on contamination and mislabeling cited above concerns SARMs specifically [P5]; nothing in this rubric extends that figure to peptides, and it should not be.
Criterion 4 (monitored path): here is where the categories actually diverge, and it is the one clean structural difference this rubric can score with confidence. A supervised telehealth path exists for compounded peptides, where a clinician reviews the individual, writes a prescription when appropriate, and tracks response through licensed pharmacies. FormBlends is one example of this model. It is named here once, as an illustration of a monitored path, not as an endorsement, not as a ranking, and there is nothing to buy or check out on this page. No comparable path exists for SARMs, per Criterion 4 above [P4].
That last line is the actual finding of this rubric. It is not that peptides are faster or safer as a blanket category, because the category is too heterogeneous to grade that way. It is that peptides include a lane with a monitored path and SARMs do not have one at all.
Where the data simply runs out
A rubric should flag its own blind spots, so here they are.
The controlled SARM benefit data tops out at 12 weeks [P1]. The harm data tops out at 21 days for suppression [P2] and five weeks for the liver case [P3]. Nobody has published controlled data on what a year or more of repeated, unsupervised cycling does to muscle, hormones, or the liver. Any claim projecting benefit out past a few months is extrapolating past the evidence, full stop, in either direction. Extending the clock does not resolve things in the compound’s favor: the favorable data does not reach that far, and the unfavorable signals already showed up earlier than the favorable data did.
Final scorecard, summarized
SARMs: pass on Criterion 1 (12-week benefit, well-documented, statistically significant [P1]). Fail on Criterion 2 (harm signals at three and five weeks, ahead of the benefit checkpoint [P2][P3][P6]). Fail on Criterion 3 (roughly half of tested retail product mislabeled or misdosed [P5]). Fail on Criterion 4 (no prescribable version exists [P4]).
Peptides: ungradable as a single line on Criteria 1 through 3, because the category spans approved drugs, compounded prescriptions, and thin-evidence research compounds, each requiring its own score. Pass on Criterion 4, in that a monitored, clinician-tracked path exists for the compounded route, which the SARM category cannot offer at all.
This is not a verdict on what anyone should take. It is a scorecard built entirely from the cited trials, case report, contamination study, and regulatory statements above. Read the caveats attached to each row before drawing a conclusion from any single cell.
Frequently asked questions
On the SARM benefit timeline, what’s the actual documented number? Twelve weeks, from a phase 2 enobosarm trial: a statistically significant, dose-dependent increase in lean body mass (P less than 0.001 at 3 mg vs placebo) plus measured improvement in physical function [P1]. That number was produced under trial monitoring with a verified product. It does not transfer to an unverified purchase or extend automatically past 12 weeks.
Does the harm data really beat the benefit data to the clock? On the published numbers, yes. Hormonal and lipid suppression showed up within 21 days (three weeks) of LGD-4033 dosing [P2], and a documented cholestatic liver-injury case occurred at five weeks of RAD-140 [P3]. Both precede the 12-week point where the lean-mass benefit was measured [P1]. That is the asymmetry this rubric is scoring.
Do peptides simply score better across the board? No, and scoring them that way would misrepresent a genuinely mixed category. Peptides range from FDA-approved drugs with solid trial data to research-status compounds with thin human evidence, so Criteria 1 through 3 have to be graded compound by compound. The one criterion peptides pass cleanly is Criterion 4: a monitored, clinician-tracked path exists for the compounded route.
Can a SARM be prescribed and monitored the way some peptides are? No. The U.S. Anti-Doping Agency states there are no FDA-approved SARMs available for prescription [P4], which means Criterion 4 fails structurally for this entire category. A monitored path generates bloodwork and adjustment over time. An unmonitored path generates no comparable record.
If the harm data is only short-term, does that mean long-term use is fine once you clear the early weeks? The evidence does not support that inference. The benefit data caps out at 12 weeks and simply does not extend further [P1]; the harm signals, by contrast, already appear at three and five weeks [P2][P3]. Stretching the timeline out does not tilt the score toward the compound, because the favorable data doesn’t reach that far and the unfavorable data arrived early.
Why can’t an online SARM buyer trust any timeline for their specific product? Because Criterion 3 fails at the market level. Testing of 44 products sold online as SARMs found only 52% contained the labeled compound, and most of those that did had the wrong dose [P5]. A timeline assumes known dose and known compound. Remove both assumptions and the timeline stops being a timeline.
References
- Enobosarm (GTx-024) produced dose-dependent, statistically significant increases in lean body mass (P less than 0.001, 3 mg vs placebo) and improved physical function over 12 weeks in 120 healthy elderly men and postmenopausal women. Double-blind, placebo-controlled phase II trial. Dalton JT, et al. Journal of Cachexia, Sarcopenia and Muscle, 2011. https://pubmed.ncbi.nlm.nih.gov/22031847/
- LGD-4033 (ligandrol) over 21 days in healthy young men produced dose-dependent suppression of total testosterone, sex hormone-binding globulin, and HDL cholesterol. Basaria S, et al. J Gerontol A Biol Sci Med Sci, 2013. https://pubmed.ncbi.nlm.nih.gov/22459616/
- A 24-year-old man developed cholestatic drug-induced liver injury after five weeks of RAD-140, peak total bilirubin 38.5 mg/dL. RAD-140 Drug-Induced Liver Injury. Ochsner Journal, 2022.
- All SARMs are investigational and not FDA-approved; there are no FDA-approved SARMs available for prescription. U.S. Anti-Doping Agency.
- Of 44 products sold online as SARMs, only 52% contained the labeled SARM, with the dose wrong in most. Van Wagoner RM, et al. JAMA, 2017.
- Products containing SARMs carry the risk of life-threatening reactions including liver damage and the potential to increase the risk of heart attack and stroke; they are unapproved drugs, not dietary supplements. U.S. Food and Drug Administration.
This scorecard does not endorse SARMs or recommend their use. SARMs are unapproved, investigational compounds with documented liver, cardiovascular, and hormonal-suppression risks, and none can be legally prescribed. Among peptides, some are prescription or compounded medications, and compounded medications are not FDA-approved finished drug products. Talk to a licensed clinician before making any decision.
Written by Elena Eriksen, health explainer. Last reviewed April 2026.
Offered for general understanding, not as advice. Check with your provider before acting.